Contraceptives fail far more often than we realize. However, statistics showing the magnitude of this unreliability are actually somewhat misleading – they usually report instances of unreliability in a given year. It is worth noting that the risk of unreliability increases over a longer period of time.
It is one of those things that makes sense if you stop and think about it. A series of interactive charts by Gregor Aisch and Bill Marsh, featured in a weekend edition of The New York Times, helps put the problem into perspective. Here is the data for three of the fifteen contraceptive methods presented in their visualization:
These charts, while not entirely accurate (see the Considerations subsection below), depict a fact that we unfortunately have little awareness regarding the unreliability of contraceptives: the longer the duration of contraceptive use - be it the pill, condoms, spermicides or similar ones - the greater the likelihood of unreliability.
The same rule applies to all games of chance that contain an element of risk. Imagine playing Russian roulette with a hundred-chamber revolver. You load one bullet into the cylinder, rotate it, move it in place and pull the trigger.
Our chances of firing a round are only 1 in 100. Significantly, the chances are only 1 in 100 with each repetition of the entire process. However, by repeating the process a greater number of times – loading the bullet, rotating the cylinder, placing it in the right site, pulling the trigger; loading, rotating, placing, pulling the trigger - the overall risk of firing the gun increases.
The same scheme applies for condoms or the pill, neither of which guarantee 100 percent effectiveness. The rule of probability indicates that both of these measures (and most other contraception methods) are likely to fail in the long term of use.
In case of hormonal contraception, unreliability is extremely often due to our irresponsible behaviour - carelessness and oversight. All you need is simply forget to fill a prescription in time, inadvertently skip the next dose of a medication, and thus significantly reduce your body's protection against unwanted pregnancy. As for condoms, on the other hand, it is extremely easy to accidentally damage them when putting on. In other words: the longer one uses a contraceptive, the more opportunities for misuse and inconsistent use.
The fact that none of us is perfect underscores the difference between what James Trussell, professor of economics and public relations at the Office of Population Research at Princeton, referred to in a 2011 report on the unreliability of contraceptives in the United States, and what he labelled "perfect use" and "typical use. " Aisch and Marsh, who used Trussell’s statistics in developing their own charts, characterize the two standards as follows:
Typical use: this is the norm, reflecting the effectiveness of any contraception method chosen by the average couple, who do not always use the method correctly or consistently (systematically).
Perfect use: this is a measure of the technical effectiveness of any method, but only if the method is applied systematically and exactly as specified. Few couples, if any, manage to achieve reliable contraceptive efficacy, especially over longer time periods.
The difference between theory and practice allows creating the chart shown below:
For condom use by heterosexual couples, the predicted number of women who include the risk of experiencing an unplanned pregnancy is 86 out of 100 per decade. As much as eighty-six percent! Just compare this to an even higher 92 percent probability of pregnancy for women in relationships using the so-called withdrawal method (also over a ten-year period). It is not hard to notice how close these figures are to each other. .
Condoms, of course, provide protection against sexually transmitted diseases, which in turn is not guaranteed by the withdrawal method, therefore these methods should not be compared to each other in absolutely every aspect. Yet, in terms of the incidence of unplanned pregnancies, the difference between the two protection measures is only 6%, which may come as quite a surprise to some people.
When using male condoms for 10 years, the difference between the pregnancy rate during perfect use (18%) and typical use (86%) is almost 70%. This is a huge result. With the exception of the ovulation method (perfect use - 26%, typical use - 94%), this is a much larger discrepancy than for any other contraceptive. According to Professor Trussell, the gap tells us something important about condoms:
The difference between the pregnancy rate during imperfect use of the method and the pregnancy rate during perfect use shows how prone to imperfect use the measure is," he explains. "The difference between the pregnancy rate during typical use and the pregnancy rate during perfect use reveals the effects (consequences) of imperfect use.
As a result - and this is perhaps the most important conclusion - the unreliability of condoms is due to imperfect use and/or inconsistent application. In other words: the risks associated with user error (or negligence) are high. This suggests the following thing - if we want contraception to be effective, we should minimize the interaction of the contraceptive user. The data clearly indicate this. Here is a chart on oral contraceptive pills, the Evra patch and the Nuvaring disc made by Aisch and Marsh:
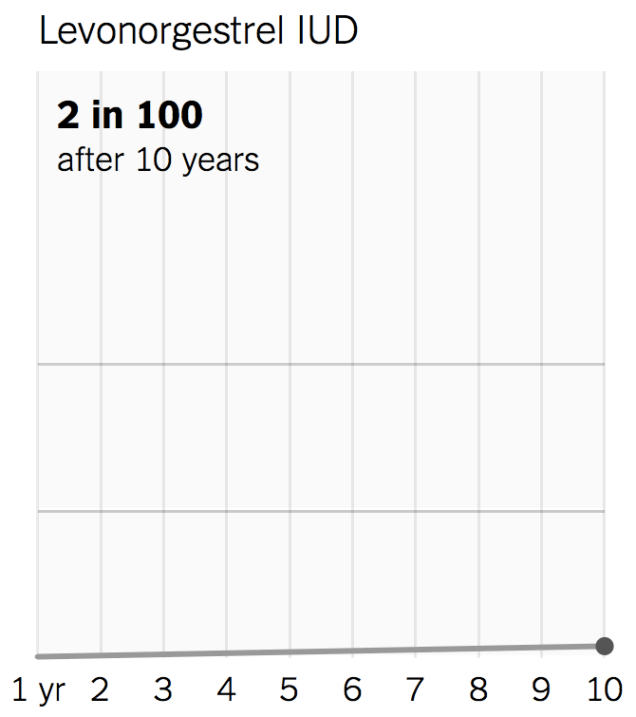
These methods of contraception, when used correctly and consistently, are predicted to result in unplanned pregnancy for only 3% of women over a period covering ten years. This is significantly lower than the projected percentage of women who have undergone sterilization, yet still at risk of becoming pregnant in the same time frame.
However, people are not perfect. We forget, misremember and misapply (use incorrectly). Having considered the foregoing, you can see that in such a case the unwanted pregnancy rate (not within a year, but over a period of at least 10 years) is not 3%, but as high as 61%. This is one of the main reasons explaining why sterilization, hormonal implants and coils are so effective – the risk of their misuse is practically zero (it is impossible to use them improperly). This is certain and undeniable. In the graph developed for an IUD containing levonorgestrel (Levornorgestrel IUD), the curve showing typical use and perfect use overlap:
There are a few important things to keep in mind when analysing the charts by Aisch and Marsh. We will breathe a sigh of relief to learn, for example, that the real probability of an unplanned pregnancy is actually lower than the "typical use" data indicate.
1. Almost all the numbers for "typical use" given in the Aisch and Marsh charts are overestimated. Here's what Prof. Trussell has to say on that matter:
[Aisch and Marsh] used my estimates of a measure's unreliability under "typical use" and "perfect use" within the first year of use to design their charts for a ten-year period. Such forecasting is good for "perfect use." But given the "typical use" does not work – the indicators are inflated. The reason for this is that an unplanned pregnancy does occur only in a small supporter group of a particular contraceptive method; within the remaining group of people, the likelihood of pregnancy becomes smaller and smaller over time. I told [Bill Marsh] this. To date, there have been no studies on this topic covering a 10-year time period, with the exception of studies on the female sterilization results. I encouraged him to use an alternate chart that would present the same point of view, but in a more efficient (and correct) way.
The chart proposed by Prof. Trussel:
Reference: Trussell J, Guthrie KA. Choosing a contraceptive: efficacy, safety, and personal considerations. w: Hatcher RA, Trussell J, Nelson AL, Cates W, Kowal D, Policar M (eds). Contraceptive Technology: Twentieth Revised Edition. New York NY: Ardent Media; 2011, s. 45-74.
2. The results originally presented by Trussell are estimates, obtained through data collected during surveys conducted among a wide range of heterosexual couples. The probability of pregnancy for most of the contraceptives considered was estimated based on data obtained in 1995 and again in 2002 – a series of National Surveys of Family Growth (NSFG) were conducted at the time. Rates of unplanned pregnancies for other contraceptive methods were calculated through other surveys and clinical trials. (For example, estimates for "typical use" of male condoms were obtained by relying on survey responses from 1995 and 2002, while the magnitude of the unplanned pregnancy problem for "perfect use" of condoms was estimated based on "only three surveys and an analysis of male condoms conforming to modern standards of design and manufacture.")
Result? These numbers cannot outline with certainty how great the probability of an unwanted pregnancy is in our case, because the only people who can tell us how consistent we remain in using the contraceptive of our choice are ourselves. Indicators tell us about the unreliability of a particular contraceptive method or, just as importantly, show us how great an ineffectiveness it can be, even when used flawlessly.
3. Estimated numbers have been adjusted for under-reporting of abortions and over-reporting of contraceptive use; these indicators, while public, do not reflect reality in a fully error-free manner. As Trussell notes:
Thus, deviations in opposite directions affect these estimates. The accepted rate for determining the incidence of pregnancy based on NSFG survey results alone appears to be too low, as the percentage of abortions (and contraceptive failure forcing the removal of an unwanted pregnancy) is underestimated, but may also be too high, as the percentage of births caused by contraceptive failure is usually overestimated. At the same time, it is important to be aware of the more serious consequences of underestimating the rate of abortions performed in this case.
4. "Typical use" described by Prof. Trussell, and our understanding of the concept are not clear, and - unless we are trying or want to get pregnant - should not be absolutely clear. Here is a comprehensive definition of "typical use" taken from the Trussell’s report:
Typical use does not mean that the contraceptive method has always been used (applied). In NSFG surveys and in most clinical trials, a woman actually "uses" a contraceptive method if she believes she is protecting herself from pregnancy with that method. Thus, in reality, typical condom use may include condom use only occasionally, and furthermore, a woman may report that she is "using" the pill, although the pack of pills she is taking ended several months ago. In short: the concept of "use" meaning "typical use" is a very flexible concept that depends solely on the individual woman's perception.
If our individual perception of the term "typical use" is closer to the definition: "I use a condom every time I have sex" than a statement: "in my nightstand I have condoms whose expiration date is over even before Barack Obama first became president of the United States," our chances of getting an unwanted pregnancy will be much lower.
The text is based on an article titled: „What Are the Real Odds That Your Birth Control Will Fail?” [http://io9.com/what-are-the-real-odds-that-your-birth-control-will-fai-1634707739]





